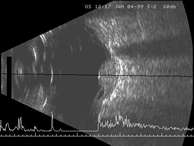
Tumours close to
the front of the eye are difficult to measure with conventional ultrasonography.
Special high-frequency probes have recently been developed, which provide
very clear views of the anterior chamber of the eye. These require the
use of a small eye-bath, filled with hypromellose, which is a viscous,
clear fluid.
Magnetic Resonance
Imaging
Magnetic resonance imaging is performed by emitting pulses of magnetism
through the body so that all the atoms spin in the same direction thereby
giving rise to electrical fields, which can then be measured and converted
into images. This type of scan produces very clear pictures of the eye,
with different tissues showing different degrees of brightness. Melanin,
for example, becomes bright with one type of MRI scan (ie, 'T1') and
dark with another type (ie, 'T2'). Although this information is helpful
in certain circumstances, there are limitations, because not all melanomas
have melanin and, conversely, not all melanotic tumours are melanomas.
Magnetic resonance
imaging is expensive and there may be a waiting list. Furthermore, the
examination can be quite stressful if the patient suffers from claustrophobia.
For these reasons, it is not performed routinely but is only reserved
for the rare instances when the diagnosis is not provided by ophthalmoscopy
and ultrasonography.
Computerized
tomography
CT scans are obtained by passing very fine x-rays through the body from
different directions and then reconstructing the results to create an
image 'slice' of the body. This type of scan does not usually provide
more information than ultrasonography, which is more convenient and
less expensive.
Biopsy
The large majority of intraocular tumours can be diagnosed quite reliably
by ophthalmoscopy and ultrasonography. Biopsy is useful for the rare
instance when there is considerable doubt about the diagnosis despite
full clinical examination.
Fine needle aspiration
biopsy
Fine needle aspiration biopsy (FNAB) is performed by passing a very
fine needle through the eye into the middle of the tumour and then gently
moving the tip of the needle backwards and forwards a few times so that
tiny tumour fragments are forced up the needle. Gentle suction can be
applied at the same time to improve the yield.
Fine needle aspiration
biopsy has the advantage of being a simple procedure from the surgical
point of view. However, the yield of tumour cells is small and may not
be enough to allow the diagnosis to be confirmed by special stains.
To ensure that an adequate specimen has been obtained it is helpful
if the pathologist can come to the operating theatre suite equipped
with a microscope.
One might imagine
that passing a needle through the retina would inevitably cause a retinal
detachment, but this complication is surprisingly rare. There is often
a mild haemorrhage, which can cause blurred vision or floaters, but
this usually resolves spontaneously in a short time.
Incisional biopsy
Incisional biopsy is performed by creating a small trapdoor directly
over the tumour and removing a small sample with scissors. This is a
more difficult procedure than fine needle aspiration biopsy, and is
usually performed under general anaesthesia, with mild or moderate lowering
of the blood pressure.
There is also a
risk of seeding tumour cells into the normal tissues around the eye
and if the tumour is not treated quickly it may spread through the opening
created by the surgery. For these reasons, a ruthenium plaque is placed
over the area of the biopsy during the same procedure, selecting the
time for which the plaque is left in place according to the diagnosis
of the tumour. For example, if pathological examination shows the tumour
to be a metastasis then the plaque is removed after delivering a dose
of about 40 Gy to the tumour summit whereas if it is a melanoma, the
exposure time is twice as long.
Excisional biopsy
Excisional biopsy involves total removal of the tumour, thereby providing
both a diagnosis and a cure. It is mostly performed if local resection
would be the treatment of choice in any case. Occasionally, if the eye
is blind, painful and painful or unsightly the most practical solution
is to remove the eye and to establish the diagnosis by pathological
examination.