This operation is
difficult, semi-experimental and controversial and therefore used as
a last resort when a tumour is located next to the optic nerve and when
it is important to conserve vision.
Conjunctival
excision
Discrete tumour nodules on the surface of the eyeball can be removed
surgically, if not too extensive. This operation is usually performed
under general anaesthesia.
Phototherapy
Laser treatment involves heating the tumour for about one minute, using
an infrared laser beam. The treatment lasts about half an hour and is
delivered under local anaesthesia on an outpatient basis.
This treatment is
suitable for small tumours, which are not more than 3 mm thick, and
which are too close to the optic nerve for radiotherapy.
Cryotherapy
Very thin tumours on the surface of the eyeball can be given 'freezing
treatment', using either a spray of liquid nitrogen or a special pencil-like
device. This treatment can be administered under local or general anaesthesia.
External beam
radiotherapy
External beam radiotherapy is indicated for choroidal haemangiomas and
metastases. These tumours respond to doses of radiation that are low
enough to be well tolerated by the eye. The equipment required for this
treatment is available at most hospitals. To reduce complications, the
treatment is given in small doses over three to four weeks. The eye
is treated from the side to avoid cataract.
Topical chemotherapy
Very thin tumours on the surface of the eye that are too extensive for
surgical removal can be treated with special drops ('weedkiller'), consisting
of Mitomycin C or 5-FU. These drops are administered on an outpatient
basis, with each course lasting between two and four weeks.
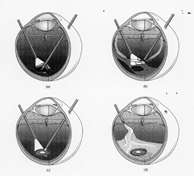
Enucleation
Removal of the eye is indicated when the chances of conserving a useful
eye are low and when the risk of complications is high.
The operation is
performed under general anaesthesia. A long-acting anaesthetic injection
is given during the anaesthesia to minimize pain during the first few
post-operative days. The enucleated eye is replaced by a bone-like ball
implant. The eye muscles are sutured to this implant so that the artificial
eye will move with the fellow eye. At the end of the operation a transparent
'conformer', similar to a rigid contact lens, is placed in the socket.
About ten weeks after surgery, this is replaced by a 'tailor-made' permanent
artificial eye, at the patient's referring hospital.
Exenteration
In very rare instances it is necessary to remove not only the eye but
also the surrounding tissues and the eyelids. A special cosmetic prosthesis
is made after the operation.